Overview
If we establish that the patient has a patent upper airway, then we need to think about:
- Ventilation
- Aspiration risk
- Secretion management
Select the Ventilation tab to continue.

Ventilation
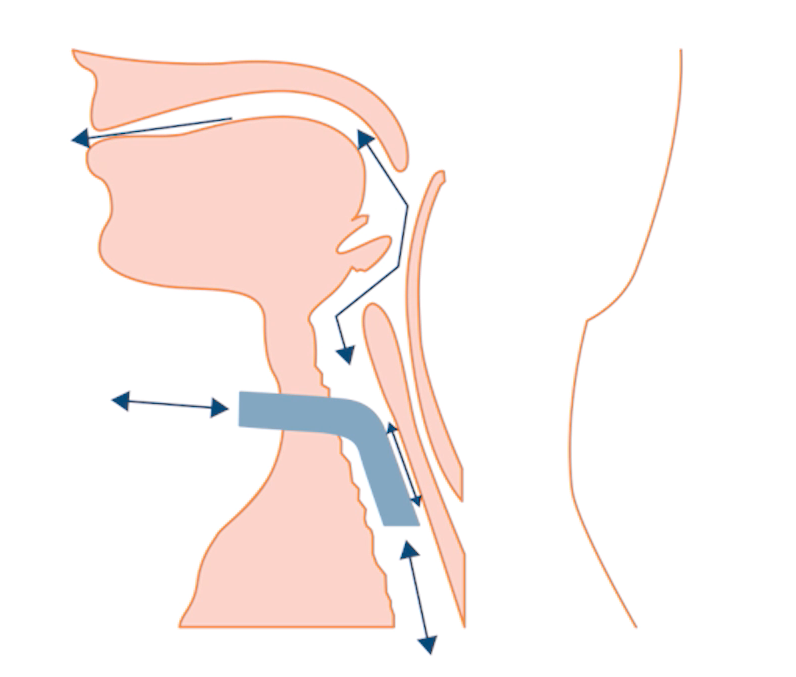
If the patient requires high airway pressures, then deflating the cuff can quickly lead to inadequate ventilation. The positive pressure gas takes the path of least resistance, and if the lungs are ‘stiff’ then a lot of gas will escape via the upper airways. Patients can fatigue quickly as their breathing will become hard work.
In addition, the reduction in intra-thoracic pressure can also impact on cardiac function and the patient should be monitored carefully for signs of physiological distress during periods of cuff deflation. Patients with high oxygen requirements must be assessed carefully, although there are no absolute cut off values.
Because of these potential problems, the multidisciplinary team must review the ventilator settings and the balance of risks and benefits from cuff deflation in ventilator-dependent patients. Often, starting for short periods (<10 minutes) and building up tolerance of cuff deflation is the best strategy. If problems are encountered, take steps to address them (treatment of heart failure for example).
Ventilator settings will usually have to be increased to allow for the gas escaping via the upper airways:
- Increased peak inspiratory pressure
- Increased inspiratory time (if the ventilator has this facility)
- A set background mandatory rate of ventilation in addition to spontaneous breaths can sometime help
The ventilator used with cuff deflation must be one that tolerates a leak from its breathing circuits. Typically, this means a ‘non-invasive’ ventilator, or selecting a setting that indicates NIV mode.
Select the Aspiration risk tab to continue.
Aspiration risk
Aspiration risk is linked to the secretion management, swallowing, coughing, laryngeal function and general condition of the patient. Any oesophageal or gastric problems can also increase the risk of aspiration of stomach contents.
However, there is a balance here between cuff deflation aimed at restoring and improving laryngeal performance (which will reduce aspiration risk) and keeping the cuff inflated to offer a degree of protection to aspiration into the lungs.
Detailed swallowing evaluation is recommended to offer an informed multidisciplinary assessment of aspiration risk and to devise strategies to improve function and reduce risk. FEES is particularly useful here – we will explore it in detail later.
Question: Does cuff deflation always increase the risk of aspiration?
Aspiration risk is linked to the secretion management, swallowing, coughing, laryngeal function and general condition of the patient. Any oesophageal or gastric problems can also increase the risk of aspiration of stomach contents.
However, there is a balance here between cuff deflation aimed at restoring and improving laryngeal performance (which will reduce aspiration risk) and keeping the cuff inflated to offer a degree of protection to aspiration into the lungs.
Detailed swallowing evaluation is recommended to offer an informed multidisciplinary assessment of aspiration risk and to devise strategies to improve function and reduce risk. FEES is particularly useful here – we will explore it in detail later.
Question: Does cuff deflation always increase the risk of aspiration?
Answer: No. It is important to note that the inflated cuff can offer some protection against this but is not a guarantee.
Fig 1 is a FEES video. It starts by showing secretions falling into the airway and being 'aspirated' through the vocal cords. Halfway through the clip, the tracheostomy tube cuff is deflated, making air flow up through the larynx. This has a number of visible effects (Table 1).
Aspiration risk is linked to the secretion management, swallowing, coughing, laryngeal function and general condition of the patient. Any oesophageal or gastric problems can also increase the risk of aspiration of stomach contents.
However, there is a balance here between cuff deflation aimed at restoring and improving laryngeal performance (which will reduce aspiration risk) and keeping the cuff inflated to offer a degree of protection to aspiration into the lungs.
Detailed swallowing evaluation is recommended to offer an informed multidisciplinary assessment of aspiration risk and to devise strategies to improve function and reduce risk. FEES is particularly useful here – we will explore it in detail later.
Question: Does cuff deflation always increase the risk of aspiration?
Answer: No. It is important to note that the inflated cuff can offer some protection against this but is not a guarantee.
Fig 1 is a FEES video. It starts by showing secretions falling into the airway and being 'aspirated' through the vocal cords. Halfway through the clip, the tracheostomy tube cuff is deflated, making air flow up through the larynx. This has a number of visible effects (Table 1).
|
Table 1 Visible effects of air flowing up through the larynx
If the patient is attached to a continuous flow of positive pressure (with CPAP in expiration) via the tracheostomy tube, then there is always a flow of gas to help to clear secretions from the larynx.
Cuff deflation remains a balance of risks, but the potential benefits for communication and early laryngeal rehabilitation is a strong argument for careful multidisciplinary assessment and consideration of early cuff deflation.
Select the Secretion management tab to continue.