Overview
For some patients, it is not possible to deflate the tracheostomy tube cuff. This is usually because high pressure ventilation is required or there is risk of ‘aspirating’ oral or gastric secretions or contents into the airway.
It is important to note that the inflated cuff can offer some protection against aspiration but is not a guarantee. Above cuff vocalisation (ACV) can help in these situations.
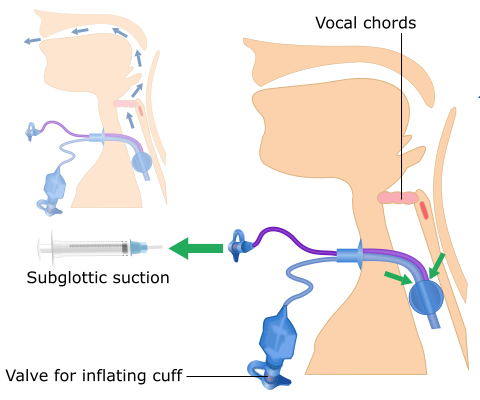
ACV has become increasingly useful as the majority of ICU patients who need a tracheostomy are having specialised subglottic suction tracheostomy tubes inserted as their primary tube (Fig 1). The subglottic ports are used to help reduce the secretions that build up above the cuff. When used as part of a bundle of care, these tubes can help reduce the incidence of ventilator-associated pneumonia.
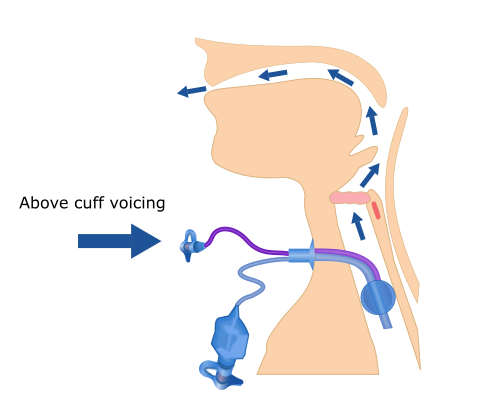
The technique for ACV uses the subglottic suction port to deliver a low flow of gas (air or oxygen) backwards, up the subglottic suction port, to exit above the cuff (Fig 2). This gas flow can then travel upwards through the trachea, pass through the vocal cords and exit via the mouth.
Select the Technique tab to continue.
Technique
Question: What proportion of ICU patients can get a voice with ACV?
Question: What proportion of ICU patients can get a voice with ACV?
Answer: ACV can result in audible vocalisation in around 80% of patients who would otherwise not be able to speak. ACV is particularly useful for those patients who cannot tolerate or be managed with a deflated tracheostomy tube cuff.
This technique, and specialised ‘talking’ tracheostomy tubes to facilitate it, have been around since the 1970s. Previously, this would require an elective change of the tracheostomy tube, but because the subglottic tubes are already in place as first choice for current ICU patients, a tube change is not required. Tube changes are difficult in the first 7-10 days following a new tracheostomy – the same period as when ACV is probably most useful.
Fig 1 is a video showing the technique.
Select the Guidelines tab to continue.
Guidelines
Guidelines and technologies for ACV are being developed as this is a relatively new technique. However, there are some principles to consider.
The NTSP does not recommend ACV unless this is performed by an appropriately trained member of healthcare staff, following a detailed risk assessment of the patient.
We recommend that subglottic and oral suction is performed prior to ACV. Warn the patient that they can expect some secretions to be ‘blown’ into their mouth. This can be unpleasant, require oral suction or lead to bad tastes or smells being experienced. Patients will frequently cough when commencing ACV as often the larynx has not been used for some time and can be sensitive.
The ACV gas flow is essentially continuous, throughout inspiration and expiration. This can take some getting used to. Research has demonstrated that ACV is safe and well tolerated and can lead to vocalisation in around 80% of patients in whom it is indicated. There may be additional benefits from promoting early trans-laryngeal gas flow that are currently not well understood.
ACV is an important option for patients who require tracheostomy cuff inflation and can lead to significant benefits from restoring the voice at these difficult times.
Select the Contraindications tab to continue.

Contraindications
Question: Can you think of any contraindication?

Question: Can you think of any contraindication?
Answer: Contraindications include:
- Upper airway obstruction or concerns about the patency of the airway
- An altered upper airway
- A new tracheostomy (typically less than 72 hours old)
- Any problems with the stoma, such as infection, bleeding or tissue breakdown
- If continuous subglottic suction is required
- A tracheostomy tube that is not in an optimal position
- A patient that is too drowsy to cooperate and coordinate vocalisation efforts
The biggest potential risk is delivery of gas into the soft tissues of the neck if the internal part of the subglottic suction port becomes displaced (associated with displacement of the whole tracheostomy tube). This can cause surgical (or subcutaneous) emphysema which can be dangerous.
Select the Safe practice tab to continue.
Safe practice
Think about how we can deliver ACV safely.
Select here to read the key points for safe practice.

Think about how we can deliver ACV safely.
Select here to read the key points for safe practice:
The NTSP considers the following points to be good practice, based on our experience and what literature there is currently available:
- Do not leave the patient un-attended during an ACV trial. We recommend limiting the trial to 15 minutes at a time, as there are concerns around drying the larynx with ACV air that are not yet fully understood
- Use a 'thumb port' (see video, or paper) so that there is only continuous gas flow when the port is actively occluded. This minimises the risk of a pressure build up should the ACV port become obstructed
- Monitor the patient continually
- Stop the trial if there is any evidence of:
- Gas escaping via the stoma, alongside the tracheostomy tube
- Pain or discomfort reported by the patient
- No voice, or no evidence of gas passing via the upper airways
- Swelling or surgical emphysema that develops at the site
- The patient becoming fatigued
A paper describing the technique can be found here.