Overview
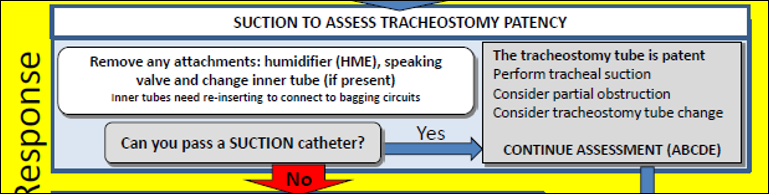
Suction the tracheostomy to assess whether it is patent (unblocked).
To do the suction, make sure any attachments are removed.
Humidifiers (HME), speaking valves or inner tubes can all become blocked.
Remember, if there is an inner tube in place and you remove it (larger tubes in older/bigger children), then you may need to replace it with a fresh or unblocked inner tube before you can use it to bag-ventilate.
If the suction catheter doesn’t pass, assume the tracheostomy is blocked.
Select the Suction catheter tab to continue.
Suction catheter
Remove any attachments, e.g. HME.
Note that paediatric tracheostomies do not usually have inner tubes.
Question: Why should you not just try and ventilate down the tube?

The suctioning technique will be explained later in this session.
Answer: Suction allows diagnosis and then treatment; removal of secretions and blood not relieved by removing the inner tube.
 The
soft suction catheter is extremely unlikely to enter the soft tissues of
the neck, and thus create a 'false passage', if the tube tip is displaced
(Fig 1). Attempts at ventilation are hazardous. If the tube tip is
displaced, surgical emphysema will develop making a difficult situation
worse.
The
soft suction catheter is extremely unlikely to enter the soft tissues of
the neck, and thus create a 'false passage', if the tube tip is displaced
(Fig 1). Attempts at ventilation are hazardous. If the tube tip is
displaced, surgical emphysema will develop making a difficult situation
worse.
An experienced responder may try gentle
ventilation, because this has the advantage of capnography, but this
cannot be recommended for all situations.
Can you pass a suction catheter?
Yes
- Perform suction, tube may be partially obstructed
- Consider tube change
- ABCDE assessment
Can you pass a suction catheter?
No
If you cannot pass a suction catheter, you have established that the tracheostomy tube is blocked or displaced.
You must now salvage the situation. The tube may be sitting in the trachea and be causing obstruction to gas flow via the upper airway.
If there is a cuff present, this should be deflated to improve the chance of oxygenating via the upper airways. Then reassess to see if your interventions have helped.